Ocular Oncology Second Opinion in Turkey — Diagnostic Review and Structured Surveillance at Eyeglow Istanbul
Independent diagnostic imaging review, multidisciplinary case discussion, written care plan and tertiary referral coordination for uveal melanoma, retinoblastoma, conjunctival and eyelid tumours. Reviewed by our ocular oncology team. We are honest: primary cancer therapy is delivered at academic tertiary referral centres — Eyeglow provides diagnosis, second opinion, navigation and post-treatment surveillance.

Verified and listed across leading directories and authorities
What is ocular oncology and what does Eyeglow offer?
Ocular oncology is the subspecialty managing cancers of the eye and orbit — uveal / choroidal melanoma, retinoblastoma, conjunctival melanoma and eyelid carcinoma. Primary therapy (plaque brachytherapy, proton beam, intra-arterial chemotherapy, immunotherapy) is delivered at academic tertiary centres. Eyeglow Health provides diagnostic imaging review, multidisciplinary case review, written care plan, tertiary referral coordination and structured post-treatment surveillance — not primary cancer therapy.
At Eyeglow Health in Istanbul, ocular oncology services are led by our ocular oncology team. Our diagnostic pathway uses Heidelberg Spectralis OCT and EDI-OCT, Optos wide-field fundus imaging, fluorescein and indocyanine green angiography, B-scan ultrasound and orbital MRI coordination — the same imaging set used in major US and European ocular oncology centres. We follow American Academy of Ophthalmology (AAO) Ocular Oncology guidelines, International Society of Ocular Oncology (ISOO) consensus and Collaborative Ocular Melanoma Study (COMS) trial principles.
The honest positioning matters in cancer care: ocular oncology medical tourism centres that overpromise primary therapy delivery without academic tertiary infrastructure are not a safe choice for patients. Eyeglow can contribute meaningfully to your care by providing a high-quality independent second opinion, coordinating referral to a true tertiary centre, and providing structured surveillance — but we do not pretend to be a comprehensive cancer centre, and we do not refer you to one that overstates its capabilities.
From first consultation to ongoing surveillance
- 01
Online ocular oncology review
You share imaging (fundus photograph, optical coherence tomography, ocular ultrasound B-scan, MRI of the orbit if available), prior biopsy or pathology reports, family history (essential for retinoblastoma) and current symptoms. Our ocular oncology team reviews the case and confirms whether the lesion is benign (choroidal naevus, retinal pigment epithelium hypertrophy), uncertain (small melanocytic lesion under observation) or malignant (uveal melanoma, retinoblastoma, conjunctival melanoma, eyelid carcinoma, lymphoma) before a quote is issued.
- 02
Comprehensive imaging in Istanbul
On day 1 we repeat or extend the imaging workup as needed: macular OCT, enhanced-depth imaging (EDI-OCT) for choroidal lesions, fundus autofluorescence, fluorescein and indocyanine green angiography, ocular ultrasound B-scan with A-scan for tumour height and internal reflectivity, anterior segment OCT for iris and ciliary body lesions, orbital MRI when needed, and metastatic workup coordination if uveal melanoma is suspected.
- 03
Multidisciplinary case review
Our ocular oncology team presents your case to a multidisciplinary team (ocular oncology, radiation oncology, medical oncology and paediatric ophthalmology for retinoblastoma) and produces a written report with the differential diagnosis, recommended primary treatment (plaque brachytherapy, proton beam radiotherapy, enucleation, intra-arterial chemo, immunotherapy, observation) and the appropriate referral centre. The report is in plain language for you and in technical detail for your home oncologist.
- 04
Referral to a tertiary ocular oncology centre
Primary ocular oncology therapy — plaque brachytherapy (I-125 or Ru-106), proton beam radiotherapy, transscleral local resection, enucleation, intra-arterial chemotherapy for retinoblastoma, intravitreal melphalan, and systemic immunotherapy (Tebentafusp / Kimmtrak FDA-approved 2022 for metastatic uveal melanoma) — is delivered at tertiary academic referral centres. Eyeglow coordinates the referral, arranges the appointment and the medical translation of records. We do not deliver the primary therapy ourselves.
- 05
Post-treatment monitoring in Istanbul
After primary treatment elsewhere — or after observation of a small choroidal lesion — we provide structured follow-up imaging at 3, 6 and 12 months: macular and tumour OCT, fundus autofluorescence, B-scan ultrasound, and metastatic surveillance coordination (liver MRI / ultrasound for uveal melanoma). Findings are reported in writing to your home oncologist.
- 06
Long-term surveillance and patient navigation
Eyeglow provides multi-year surveillance coordination, second-opinion review at any disease progression, and patient navigation services (translation, scheduling at tertiary centres, family support). Many uveal melanoma patients require lifelong surveillance for metastatic disease; we coordinate this with your home oncology team without trying to replace them.
Uveal Melanoma vs Retinoblastoma vs Conjunctival vs Eyelid Tumour
Each ocular cancer has different age distribution, first-line treatment and prognosis. Here is how Eyeglow contributes to each pathway:
| Aspect | Uveal melanoma | Retinoblastoma | Conjunctival | Eyelid tumour |
|---|---|---|---|---|
| Tumour type | Uveal melanoma (choroidal, ciliary body, iris) | Retinoblastoma (paediatric) | Conjunctival melanoma / squamous cell carcinoma | Eyelid tumour (BCC, SCC, sebaceous carcinoma) |
| Typical age | Adults 50–70 | Children under 5 | Adults 50+ | Adults 60+ |
| First-line treatment | Plaque brachytherapy (I-125 / Ru-106), proton beam | Intra-arterial chemotherapy, intravitreal melphalan, focal laser / cryo | Wide local excision + cryotherapy or topical mitomycin C | Mohs micrographic surgery or wide excision |
| Eye preservation rate | 85–90% with plaque brachytherapy | 90%+ with modern chemoreduction | Variable — depends on size | 95%+ with reconstructive surgery |
| Metastatic risk | 30–50% lifetime (liver predominant) | Rare with early treatment | Moderate | Low (BCC) to high (sebaceous, SCC) |
| Eyeglow role | Second opinion + monitoring + referral | Family imaging review + referral | Diagnostic confirmation + referral | Diagnostic review + referral to oculoplastic surgeon |
Personalised pricing
Every treatment plan is priced individually after your consultation and imaging review. Request a written, all-inclusive quote — clear, itemised, and with no obligation.
Request a written quoteWhat's included in your ocular oncology package
Included in package
- Comprehensive ocular oncology consultation (90 minutes)
- Diagnostic imaging review: OCT, EDI-OCT, fundus photo, autofluorescence, FA, ICGA, B-scan ultrasound
- Multidisciplinary case review (ocular oncology + radiation + medical oncology + paediatric specialist as needed)
- Written care plan in plain language (patient version) and technical detail (oncologist version)
- Multidisciplinary referral arrangement to tertiary academic centre when needed
- 5-star hotel — 3 nights
- VIP airport transfers (return)
- Translation of medical records into English / German / Russian / French / Spanish / Arabic as needed
- 3, 6 and 12-month structured surveillance visits with OCT and B-scan
- Multilingual oncology coordinator — 24/7
- Complication insurance for any imaging procedure performed at Eyeglow — covers eligible adverse events during your visit (issued in line with the Turkish Ministry of Health International Health Tourism Authority Certificate)
Paid separately
Items below are delivered by tertiary referral centres and billed directly by them — Eyeglow does not add mark-up.
- Flights to/from Istanbul
- Personal expenses
- Tertiary primary cancer therapy — plaque brachytherapy, proton beam radiotherapy, enucleation, intra-arterial chemotherapy, immunotherapy — all delivered at referral centre and billed by the centre directly
- Systemic chemotherapy or immunotherapy treatment courses
- Liver MRI or PET-CT for metastatic surveillance (quoted by imaging centre)
- Oncology-related medications
- Travel insurance (flight cancellation, baggage, general trip cover) — separate from the complication policy above; your coordinator can recommend a provider at no markup
The surgeons who will care for you
Your case is reviewed by our ocular oncology team at our partner accredited hospital in Istanbul. Their training and sub-specialty focus are shown below.
Medically reviewed by Assoc. Prof. Dr. Muhammet Derda Özer, FICO

Assoc. Prof. Dr. Muhammet Derda Özer, FICO
Operating Surgeon
Specialises in ocular oncology, vitreoretinal diseases, cataract, refractive, corneal transplantation, glaucoma and pediatric ophthalmic surgery — more than 30,000 ophthalmic operations across a 14-year clinical career.
View full profile
Op. Dr. Önder Aslan
Operating Surgeon
Board-certified ophthalmologist whose surgical practice spans anterior-segment procedures with oculoplastic and retinal sub-specialties — cataract, refractive, eyelid surgery and pediatric eye examinations including retinopathy of prematurity.
View full profile
Op. Dr. Muhammed Talha Sadık
Operating Surgeon
Board-certified ophthalmologist working across vitreoretinal disease, refractive, cataract and glaucoma surgery, with an active anterior- and posterior-segment surgical caseload.
View full profileSurgical outcomes from our own cases
The images below are from ocular surface tumour cases managed by our surgical team in Istanbul — documented before treatment and after surgical excision with ocular surface reconstruction. They are shared to illustrate the kind of conditions our team treats, not as a guarantee of any individual outcome.
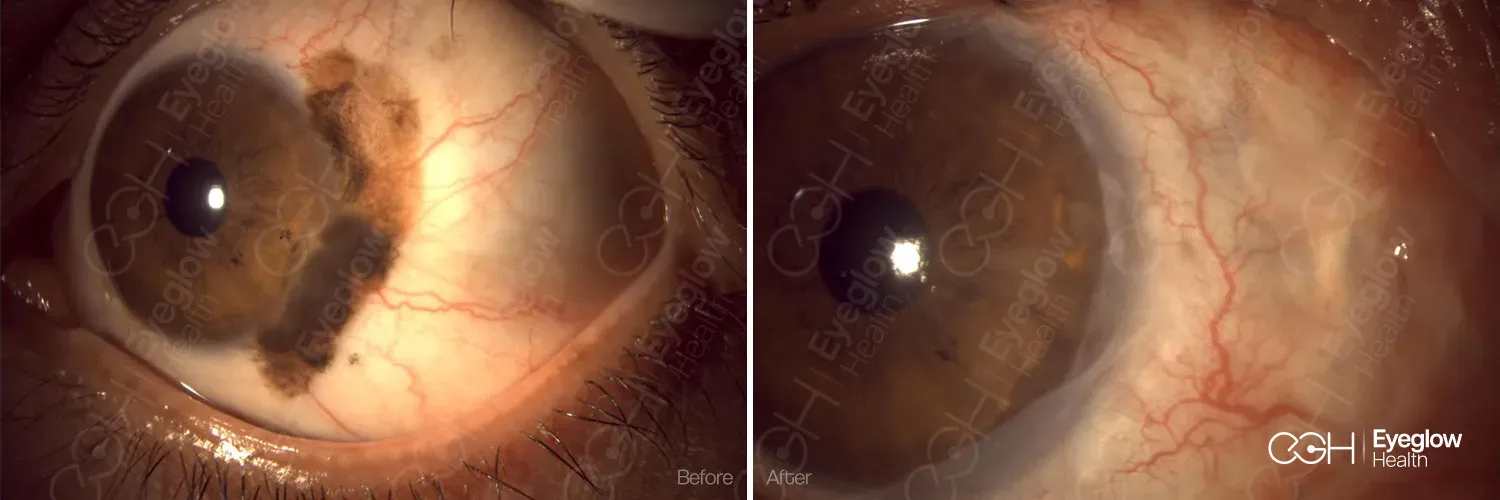
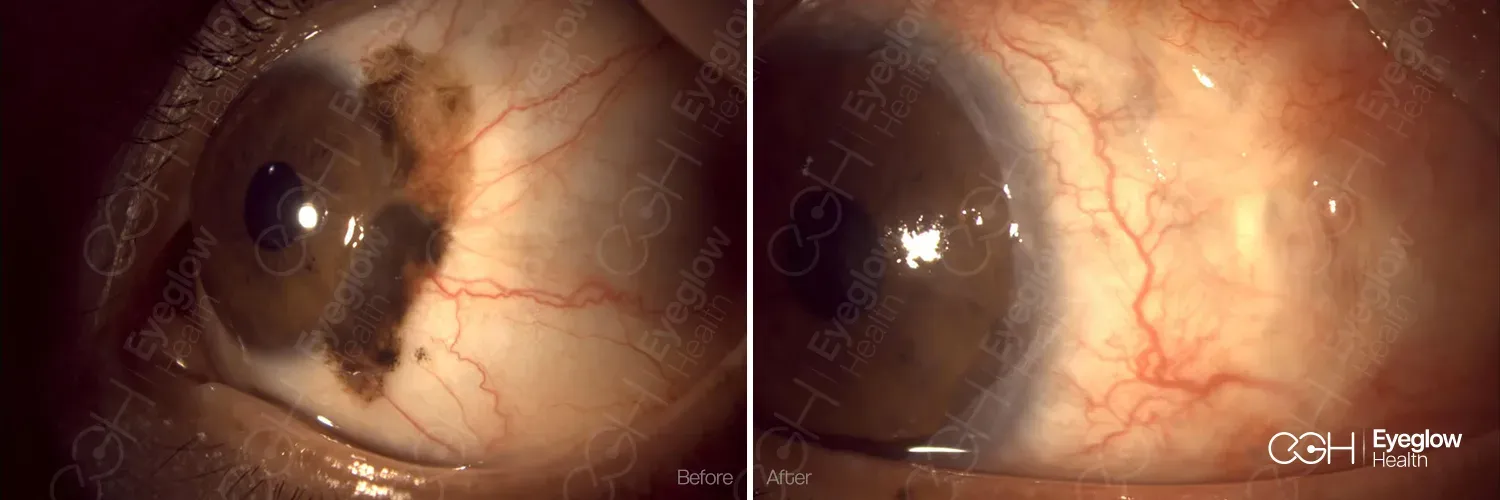
Clinical images are published with documented patient consent and are from procedures performed by our own surgical team. Individual results vary with tumour type, stage and ocular surface condition; these images do not represent a promised result for any patient.
Is Eyeglow ocular oncology service right for you?
You may benefit from our service if
- You have a newly diagnosed or suspected ocular malignancy (uveal / choroidal melanoma, retinoblastoma, conjunctival or eyelid tumour) and want an independent specialist second opinion.
- You have a small choroidal melanocytic lesion that needs serial imaging surveillance (3, 6, 12-month monitoring).
- You have completed primary cancer therapy elsewhere and need ongoing structured follow-up with OCT, fundus and metastatic surveillance coordination.
- You want multidisciplinary case review (ocular oncology + radiation oncology + medical oncology) and a written care plan transferable to your home oncologist.
- You need referral coordination to a tertiary academic centre for primary therapy (plaque brachytherapy, proton beam, enucleation, intra-arterial chemo) and want a specialist navigator to manage scheduling and translation.
A different pathway may be safer if
- You require urgent primary cancer therapy within days — you should attend your nearest tertiary academic oncology centre directly without delay.
- You expect Eyeglow to deliver primary brachytherapy, proton beam, intra-arterial chemo or systemic immunotherapy — these are tertiary procedures that we coordinate referral for, but do not deliver ourselves.
- You expect a single second-opinion visit to replace ongoing specialist oncology care — uveal melanoma surveillance is lifelong.
- You have non-ocular cancer that incidentally affects the eye (e.g. metastatic disease, paraneoplastic syndrome) — you should be cared for by your primary oncologist.
Disclaimer. Information on this page is consistent with American Academy of Ophthalmology (AAO) Ocular Oncology Preferred Practice Pattern, International Society of Ocular Oncology (ISOO) consensus, the Collaborative Ocular Melanoma Study (COMS Trial), the International Retinoblastoma Staging System (IRSS) and FDA approvals including Tebentafusp / Kimmtrak (January 2022). It is educational and not a clinical recommendation. Ocular cancer diagnosis and treatment require a multidisciplinary specialist team; Eyeglow Health provides diagnostic imaging, second opinion, multidisciplinary review and referral coordination — primary cancer therapy is delivered at tertiary academic referral centres.
What second opinion and surveillance can and cannot do
Independent ocular oncology review has clear limitations. We list them here transparently:
Diagnostic uncertainty
Small choroidal melanocytic lesions sit on a spectrum from clearly benign naevus to early melanoma; certainty often requires 6 to 12 months of serial imaging surveillance. Our second opinion contributes to this assessment but does not replace the longitudinal data your home ophthalmologist generates over time. We are transparent when uncertainty exists.
Imaging or diagnostic procedure complications
Standard ocular imaging (OCT, fundus photography, autofluorescence) is non-invasive. Fluorescein angiography carries a low rate of nausea (5–10%), mild allergic reaction (<0.5%) and very rare anaphylaxis (<0.01%). B-scan ultrasound is non-invasive and involves no radiation exposure. We screen for contrast allergies before any angiographic procedure.
Treatment outcomes depend on the referral centre
Once we refer you to a tertiary centre for plaque brachytherapy, proton beam or surgery, the outcome of that treatment is determined by the referral centre — not by Eyeglow. We choose referral centres on the basis of specialist accreditation, published outcomes and patient experience, and we transparently explain the risk profile of each option, but we cannot guarantee the result of treatment delivered elsewhere.
Metastatic surveillance limitations
Uveal melanoma has a 30 to 50 percent lifetime metastatic risk (liver predominant). Even with optimal follow-up, metastasis can develop in patients with adverse genetic features (monosomy 3, BAP1 mutation, class 2 gene expression). We coordinate metastatic surveillance with liver MRI / ultrasound and PET-CT according to risk profile but cannot eliminate this risk through monitoring alone.