Retinal Vitrectomy Surgery in Turkey — 25G / 27G Microincision PPV at Eyeglow Istanbul
Retina-specialist-led vitreoretinal surgery using the Alcon Constellation and DORC EVA microincision platforms for retinal detachment, macular hole, epiretinal membrane, vitreous haemorrhage and diabetic vitrectomy. Every case is reviewed by our retina surgical team and includes a written quote, complication insurance and a year of structured OCT follow-up.
Verified and listed across leading directories and authorities
What is a retinal vitrectomy?
Pars plana vitrectomy (PPV) is a microsurgical procedure to remove the vitreous gel from inside the eye, repair the retina, and replace the vitreous with a saline solution, gas bubble or silicone oil. Modern 25-gauge / 27-gauge microincision vitrectomy uses three sub-millimetre trans-conjunctival ports and takes 45 to 90 minutes per eye under topical anaesthetic with sedation.
At Eyeglow Health in Istanbul, vitrectomy is performed with the Alcon Constellation Vision System and DORC EVA platforms — the same equipment used in major US, UK and European vitreoretinal centres. Treatment plans are tailored to the indication: retinal detachment, full-thickness macular hole, epiretinal membrane (macular pucker), non-clearing vitreous haemorrhage, proliferative diabetic retinopathy and vitreomacular traction each have different surgical techniques, tamponade choices and posturing schedules.
Vitrectomy is a high-acuity intraocular procedure and is not appropriate for everyone. Stable asymptomatic membranes, active ocular infection, severe medical comorbidity, or patients unable to maintain posturing all require a different approach. That assessment belongs to a vitreoretinal surgeon who has personally reviewed your macular OCT, wide-field fundus imaging and visual acuity history — not to a marketing brochure.
From first consultation to recovery at home
- 01
Online retina review
You share your most recent macular OCT, fundus photograph, fluorescein angiography (if available) and any prior retinal notes. Our retina surgical team reviews your case and confirms the indication (detachment, macular hole, epiretinal membrane, vitreous haemorrhage, diabetic retinopathy or vitreomacular traction) — and what positioning will be needed after surgery — before a quote is issued.
- 02
Pre-operative imaging in Istanbul
On day 1 we repeat macular OCT, wide-field fundus imaging, B-scan ultrasonography (if media are opaque), endothelial cell count and a complete dilated retinal examination. These confirm the exact pathology, the extent of any retinal break or membrane, and whether a gas tamponade or silicone oil will be needed at the end of surgery.
- 03
Personalised surgical plan
Our retina surgical team explains the surgery in plain language: which membrane will be peeled, whether endolaser will be applied, what tamponade (SF6, C3F8 or silicone oil) will be used, and the post-operative posturing schedule. You sign consent only after every question has been answered.
- 04
Pars plana vitrectomy (45–90 minutes per eye)
25G or 27G microincision vitrectomy — three sub-millimetre trans-conjunctival ports are placed through the pars plana, the vitreous gel is removed with the Constellation or EVA vitrectomy platform, the retina is repaired (ILM peel, ERM peel, endolaser to retinal breaks, drainage of subretinal fluid as needed), and the eye is filled with a gas bubble or silicone oil tamponade according to the indication. Performed under topical anaesthetic with sedation, or a peribulbar block.
- 05
Day 1 and weekly reviews
A clear protective shield is worn at night for the first 2 weeks. You return on day 1, day 7, day 14 and again before flying. If you have a gas tamponade you must remain face-down or in lateral positioning for the prescribed period (typically 3–7 days for macular hole, 1–3 days for retinal detachment) and you cannot fly until the gas bubble dissolves — usually 2 weeks for SF6 and 6 to 8 weeks for C3F8.
- 06
One-year structured aftercare
Scheduled OCT and fundus reviews at one, three, six and twelve months. Visual recovery continues throughout the first 6 to 12 months as the macula remodels. If silicone oil was used, removal is scheduled at 3 to 6 months as a second-stage procedure (priced separately). Your coordinator stays the same throughout.
Vitrectomy by indication — what is repaired and how
Vitrectomy is one operation with many indications. The surgical steps, tamponade choice and recovery profile depend on the specific pathology:
| Aspect | Retinal detachment | Macular hole | Epiretinal membrane | Vitreous haemorrhage / diabetic |
|---|---|---|---|---|
| Indication | Retinal detachment (rhegmatogenous, tractional, exudative) | Full-thickness macular hole | Epiretinal membrane / macular pucker | Vitreous haemorrhage, diabetic retinopathy, vitreomacular traction |
| Typical surgery time | 60–90 min | 45–60 min | 45–60 min | 45–90 min (depends on retinopathy severity) |
| ILM / ERM peel | Sometimes | Always (ILM peel) | Always (ERM ± ILM) | Variable |
| Tamponade used | SF6 gas, C3F8 gas, or silicone oil | C3F8 gas (3–6 weeks) | Air or no tamponade | Usually none; gas if peripheral break |
| Post-op posturing | 1–3 days | 3–7 days face-down | None routinely | None routinely |
| Visual recovery (median) | 3–12 months | 3–6 months (90%+ closure rate) | 3–6 months (70–80% acuity gain) | 4–12 weeks once media clear |
Vitrectomy pricing
All-inclusive Eyeglow package pricing. Your final, personalised quote is confirmed after imaging review — with no obligation.
| Procedure | Eyeglow price (all-inclusive) |
|---|---|
| Retinal Vitrectomy Surgery (PPV) — per eye, all-inclusive | €4,000 – €6,000 |
What's included in your vitrectomy package
Included in package
- Pre-op imaging (macular OCT, wide-field fundus, B-scan, endothelial cell count, fluorescein angiography if needed)
- Retina-specialist consultation + surgical plan review
- 25G / 27G microincision pars plana vitrectomy (Constellation or EVA platform)
- ILM / ERM peel as indicated, endolaser to retinal breaks, drainage of subretinal fluid
- Tamponade — SF6 or C3F8 gas (silicone oil quoted separately if removal needed)
- 5-star hotel — 7 nights (longer stays available for complex cases)
- VIP airport transfers (return)
- All post-op drops + aftercare kit + posturing equipment if required
- Day-1, day-7, day-14, 1m, 3m, 6m, 12m follow-up with OCT and fundus review
- Multilingual retina coordinator — 24/7
- Complication insurance — covers eligible post-operative medical complications during the recovery period at our partner accredited hospital (issued in line with the Turkish Ministry of Health International Health Tourism Authority Certificate)
Paid separately
Items below are not part of the medical package — your coordinator helps you arrange them at no markup.
- Flights to/from Istanbul
- Personal expenses
- Silicone oil removal — quoted separately as a second-stage procedure at 3 to 6 months
- Cataract surgery — vitrectomy accelerates cataract development; ~50–80% of patients require subsequent cataract surgery within 12 to 24 months, quoted separately
- Anti-VEGF intravitreal injections for ongoing diabetic or AMD management — billed per injection
- Unrelated medical treatments
- Travel insurance (flight cancellation, baggage, general trip cover) — separate from the medical complication policy above; your coordinator can recommend a provider at no markup
The surgeons who will care for you
Your procedure is carried out by our retina surgical team at our partner accredited hospital in Istanbul. Their training and sub-specialty focus are shown below.
Medically reviewed by Assoc. Prof. Dr. Muhammet Derda Özer, FICO

Assoc. Prof. Dr. Muhammet Derda Özer, FICO
Operating Surgeon
Specialises in ocular oncology, vitreoretinal diseases, cataract, refractive, corneal transplantation, glaucoma and pediatric ophthalmic surgery — more than 30,000 ophthalmic operations across a 14-year clinical career.
View full profile
Op. Dr. Önder Aslan
Operating Surgeon
Board-certified ophthalmologist whose surgical practice spans anterior-segment procedures with oculoplastic and retinal sub-specialties — cataract, refractive, eyelid surgery and pediatric eye examinations including retinopathy of prematurity.
View full profile
Op. Dr. Muhammed Talha Sadık
Operating Surgeon
Board-certified ophthalmologist working across vitreoretinal disease, refractive, cataract and glaucoma surgery, with an active anterior- and posterior-segment surgical caseload.
View full profileVitrectomy outcomes from our own cases
The images below are from vitreoretinal surgery cases managed by our retina team in Istanbul — documented before treatment and after surgical repair, alongside intra-operative clinical imaging. They are shared to illustrate the conditions our team treats, not as a guarantee of any individual outcome.
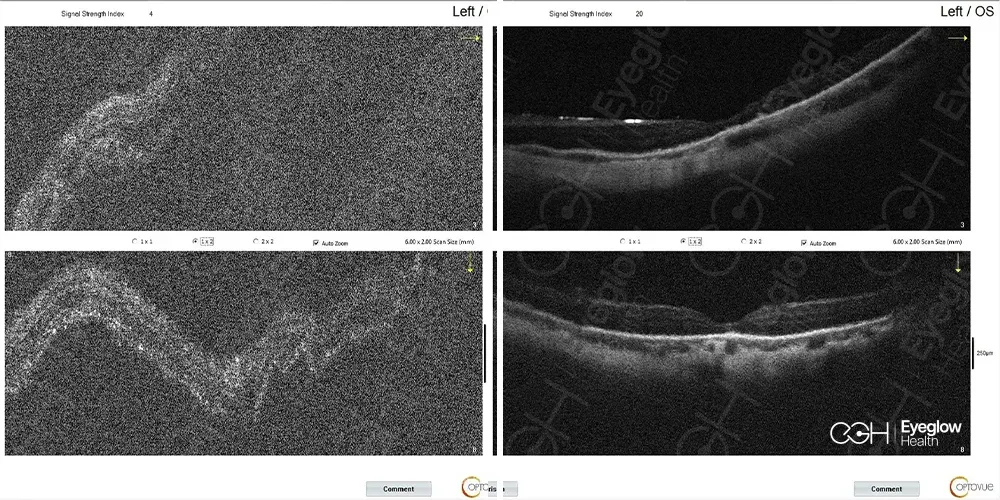
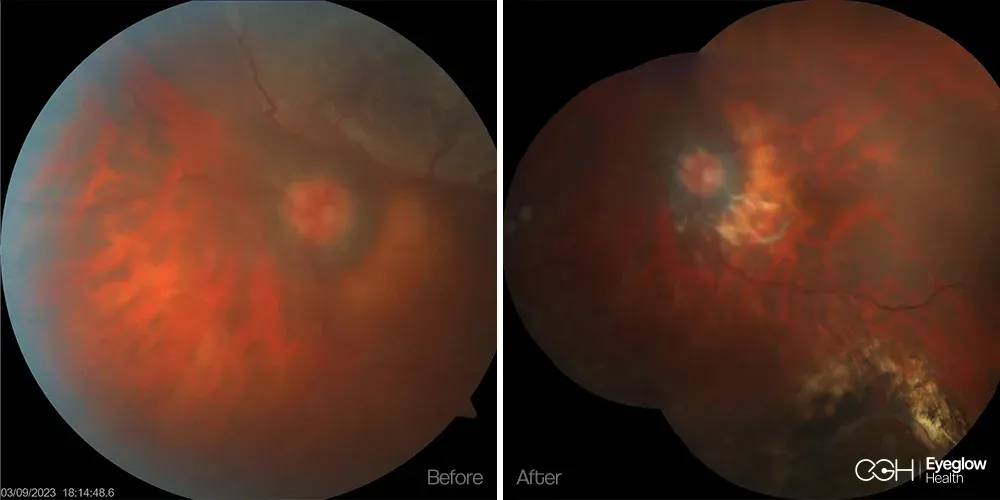
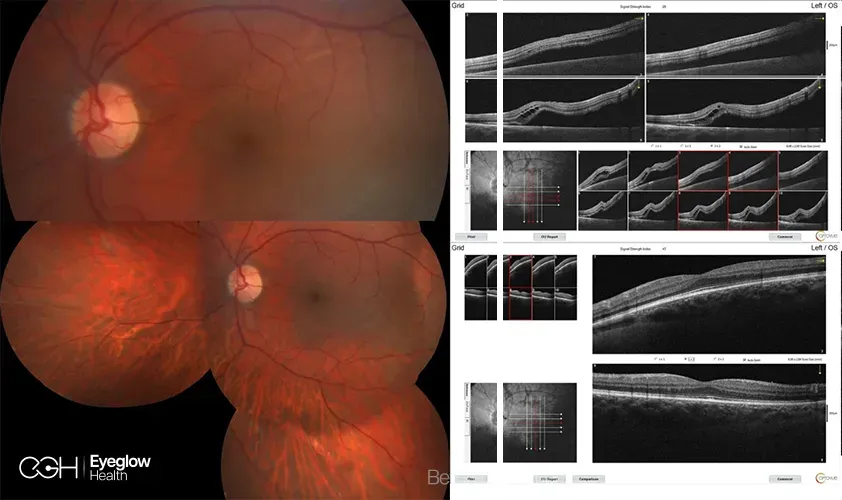
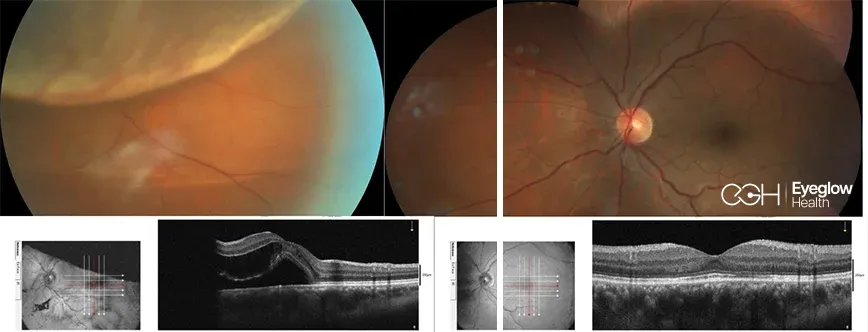
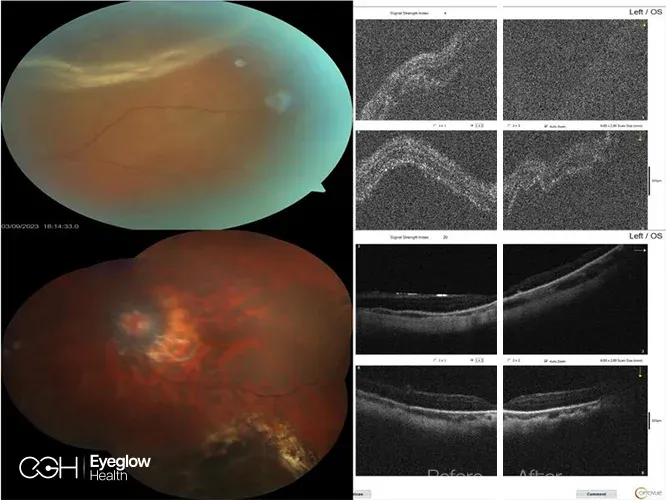
Clinical images are published with documented patient consent and are from procedures performed by our own retina team. Individual results vary with retinal condition and disease stage; these images do not represent a promised result for any patient.
Are you a candidate for vitrectomy?
You may be a good candidate if
- You have a confirmed retinal detachment requiring repair (rhegmatogenous, tractional or exudative).
- You have a full-thickness macular hole confirmed on OCT (stages 2–4) and want a single-stage surgical closure.
- You have an epiretinal membrane (macular pucker) with measurable visual acuity loss or metamorphopsia distorting daily reading.
- You have a non-clearing vitreous haemorrhage limiting your ability to drive or work after 2–3 months of observation.
- You have proliferative diabetic retinopathy with vitreous haemorrhage or tractional retinal detachment requiring vitrectomy.
- You can commit to the posturing schedule (typically 3–7 days face-down for macular hole) and to a 2 to 6-week non-flying period if gas tamponade is used.
A different pathway may be safer if
- Active ocular infection (endophthalmitis, severe uveitis) — must be controlled medically before any surgical intervention.
- Stable, asymptomatic epiretinal membrane with preserved acuity — observation is the appropriate plan.
- Recent intravitreal anti-VEGF injection within 7 days (timing must be coordinated).
- Significant medical comorbidity preventing safe sedation or block anaesthesia (assessed case-by-case).
- Patients unable to maintain post-operative posturing (frailty, severe musculoskeletal disease) — alternative tamponade or staged approach assessed individually.
Disclaimer. Information on this page is consistent with American Academy of Ophthalmology (AAO) Retina & Vitreous Preferred Practice Pattern, American Society of Retina Specialists (ASRS) consensus, Royal College of Ophthalmologists (RCO) UK vitreoretinal audit, and FDA-approved 25G / 27G microincision platforms (Alcon Constellation, DORC EVA). It is educational and not a clinical recommendation. The only reliable way to know whether vitrectomy is the right option for your eye is a vitreoretinal-specialist evaluation based on macular OCT, fundus examination and visual acuity history.
Realistic outcomes — the risks that actually matter
Every vitreoretinal procedure has measurable risks. We list them here in the same plain language our surgical team uses in your consultation:
Post-vitrectomy cataract
The most common late event after vitrectomy in patients with their natural lens. Approximately 50 to 80 percent of phakic patients develop a visually significant cataract within 12 to 24 months — independent of the vitrectomy result. Treated with routine cataract surgery (Smart Lens or monofocal IOL) when it becomes symptomatic.
Retinal redetachment
Around 5 to 10 percent of retinal detachments require a second surgery, typically because of proliferative vitreoretinopathy (PVR) — scar tissue contraction inside the eye. Anatomic success after second surgery exceeds 90 percent in published series.
Elevated intraocular pressure
Common in the first 1–2 weeks especially after gas tamponade; managed with topical medication. Persistent glaucoma is uncommon (<5%) and treated with standard glaucoma protocols.
Endophthalmitis (intraocular infection)
Rare — published incidence below 0.1% with 25G/27G microincision vitrectomy and modern aseptic technique. Detected on day-1 review and treated immediately with intravitreal antibiotics if it ever occurs.