EVO ICL Surgery in Turkey — Reversible Phakic Lens Implant at Eyeglow Istanbul
STAAR Surgical EVO ICL implantation — the FDA-approved phakic intraocular lens for high myopia, thin corneas and dry eye patients who are not candidates for LASIK. Led by our refractive surgical team. Reversible refractive surgery, written quote, complication insurance and a year of structured aftercare.
Verified and listed across leading directories and authorities
What is EVO ICL & phakic lens implantation?
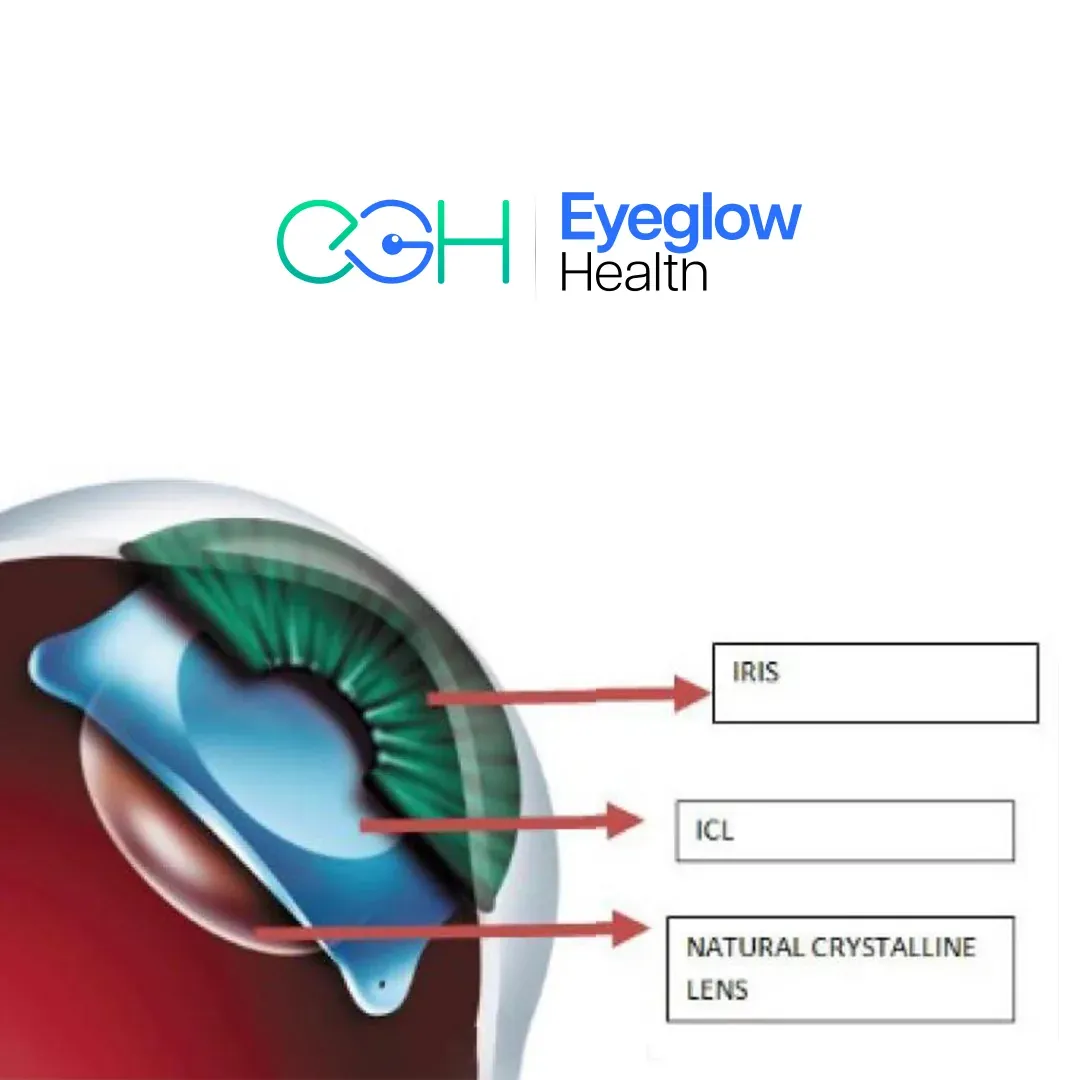
EVO ICL (Implantable Collamer Lens) is a phakic intraocular lens placed between the iris and the natural lens to correct myopia, hyperopia and astigmatism — without removing any corneal tissue or replacing the natural lens. The procedure takes 15 to 20 minutes per eye, is fully reversible, and gives functional vision within 24 hours.
At Eyeglow Health in Istanbul, EVO ICL is performed with the FDA-approved STAAR Surgical EVO Visian platform (US approval March 2022; CE-marked in Europe since 2011). The lens is made of Collamer — a proprietary collagen-copolymer biocompatible with the eye for decades, with peer-reviewed safety data extending past 10 years (Alfonso 2019; Igarashi 2014). Each lens is custom-ordered to your individual eye after biometry — sizing matters as much as power, and STAAR offers four diameters (12.1, 12.6, 13.2, 13.7 mm) to match your corneal anatomy.
EVO ICL is the appropriate refractive choice for several patient profiles where LASIK is not safe: high myopia (–10 D and above), thin corneas, moderate-to-severe dry eye, or patients who want a reversible refractive option in case their visual needs change later in life. It is not suitable for everyone — shallow anterior chambers, low endothelial cell counts, narrow-angle glaucoma or early cataract all require a different pathway. That assessment belongs to a surgeon who has personally reviewed your anterior segment OCT and endothelial cell count, not to a marketing brochure.
From first consultation to recovery at home
- 01
Online consultation
You share recent prescription, prior corneal topography (if available) and any prior LASIK / contact-lens history. Our refractive surgical team reviews your case and confirms whether your prescription range, anterior chamber depth and endothelial cell count make ICL the right choice over LASIK or SMILE — before a quote is issued.
- 02
Pre-operative imaging in Istanbul
On day 1 we measure your anterior chamber depth (must be ≥2.8 mm), white-to-white horizontal corneal diameter (for ICL sizing — 12.1, 12.6, 13.2 or 13.7 mm), endothelial cell count (must be ≥2,200 cells/mm²), pupil dynamics, IOL Master biometry and macular OCT. These are the inputs that determine ICL power and size — not your prescription alone.
- 03
ICL ordered to your eye
Once measurements are confirmed, our refractive surgical team orders your EVO ICL (or Toric EVO ICL if astigmatism above 1.0 D) directly from STAAR Surgical. The lens is custom-manufactured to your exact dioptric power and corneal diameter. Delivery typically takes 7–14 days, so most patients schedule the procedure 2–3 weeks after the initial consultation.
- 04
The procedure (15–20 minutes per eye)
Both eyes are treated 1–7 days apart. A 2.8 mm corneal incision is created, the foldable EVO ICL is injected into the posterior chamber and centred between the iris and the natural lens. The EVO platform has a central 360 µm CentraFLOW port — so a peripheral iridotomy is no longer needed, unlike the older V4 Visian ICL. Topical anaesthetic; mild sedation available.
- 05
Day 1 and day 7 reviews
You return the morning after surgery and again before flying home. Most patients see clearly enough to drive within 24 hours; visual recovery is faster than LASIK because the cornea is not reshaped — vision corrects through an internal lens, not surface tissue. A protective shield is worn for the first two nights.
- 06
One-year structured aftercare
Scheduled video reviews at one, three, six and twelve months — with annual endothelial cell-count monitoring afterwards. Your coordinator stays the same. Because ICL is reversible, if your prescription drifts later in life (e.g. presbyopia in your 50s), the ICL can be removed and a Smart Lens implanted instead — a unique advantage of the phakic IOL pathway.
EVO ICL vs LASIK vs SMILE vs Smart Lens
EVO ICL is one of four refractive pathways at Eyeglow. The right choice depends on prescription range, corneal anatomy and whether reversibility matters to you:
| Aspect | EVO ICL | LASIK | SMILE | Smart Lens |
|---|---|---|---|---|
| Best for | High myopia (–3 to –20 D), thin cornea, dry eye, athletes | Mild-to-moderate myopia, hyperopia, astigmatism with healthy thick cornea | Moderate myopia, thinner cornea than LASIK threshold | Patients over 50, cataract or presbyopia correction |
| Reversibility | ✓ Lens can be removed or exchanged | ✗ Permanent corneal reshape | ✗ Permanent corneal lenticule removal | ✗ Natural lens removed permanently |
| Cornea preserved | ✓ No corneal tissue removed | ✗ Stromal ablation + flap | ✗ Stromal lenticule | ✓ Cornea preserved, lens replaced |
| Recovery time | 24 hours functional | 24–48 hours | 4–6 days | 24–72 hours |
| Dry eye risk | Minimal (no nerve transection) | Moderate (flap nerve transection) | Lower than LASIK | Minimal |
| Night vision quality | Excellent (no halos in EVO) | Mild halos initially | Mild halos initially | Halos with multifocal IOLs |
| Upper prescription limit | Up to –18 to –20 D myopia | ~–10 D myopia | ~–10 D myopia | Any (lens-based) |
EVO ICL pricing
All-inclusive Eyeglow package pricing. Your final, personalised quote is confirmed after imaging review — with no obligation.
| Procedure | Eyeglow price (all-inclusive) |
|---|---|
| EVO ICL Surgery — per eye, all-inclusive | €4,500 – €6,000 |
What's included in your EVO ICL package
Included in package
- Pre-op imaging (anterior chamber depth, white-to-white, endothelial cell count, pupil dynamics, IOL Master biometry, macular OCT)
- Surgeon-led consultation + ICL sizing review (our refractive surgical team)
- EVO ICL or Toric EVO ICL — STAAR Surgical custom-ordered to your eye
- Phakic IOL implantation (both eyes, scheduled 1–7 days apart)
- 5-star hotel — 4 nights
- VIP airport transfers (return)
- All post-op drops + aftercare kit
- Day-1, day-7, 1m, 3m, 6m, 12m follow-up reviews
- Annual endothelial cell-count monitoring (year 1 included; year 2+ remote review)
- Multilingual coordinator — 24/7
- Complication insurance — covers eligible post-operative medical complications during the recovery period at our partner accredited hospital (issued in line with the Turkish Ministry of Health International Health Tourism Authority Certificate)
Paid separately
Items below are not part of the medical package — your coordinator helps you arrange them at no markup.
- Flights to/from Istanbul
- Personal expenses
- Lens exchange in case of prescription drift after year 5 (quoted separately if ever required)
- Unrelated medical treatments
- Travel insurance (flight cancellation, baggage, general trip cover) — separate from the medical complication policy above; your coordinator can recommend a provider at no markup
The surgeons who will care for you
Your procedure is carried out by our refractive surgical team at our partner accredited hospital in Istanbul. Their training and sub-specialty focus are shown below.
Medically reviewed by Assoc. Prof. Dr. Muhammet Derda Özer, FICO

Assoc. Prof. Dr. Muhammet Derda Özer, FICO
Operating Surgeon
Specialises in ocular oncology, vitreoretinal diseases, cataract, refractive, corneal transplantation, glaucoma and pediatric ophthalmic surgery — more than 30,000 ophthalmic operations across a 14-year clinical career.
View full profile
Op. Dr. Önder Aslan
Operating Surgeon
Board-certified ophthalmologist whose surgical practice spans anterior-segment procedures with oculoplastic and retinal sub-specialties — cataract, refractive, eyelid surgery and pediatric eye examinations including retinopathy of prematurity.
View full profile
Op. Dr. Muhammed Talha Sadık
Operating Surgeon
Board-certified ophthalmologist working across vitreoretinal disease, refractive, cataract and glaucoma surgery, with an active anterior- and posterior-segment surgical caseload.
View full profileAre you a candidate for EVO ICL?
You may be a good candidate if
- You are aged 21 to 45 with a stable prescription for at least one year.
- Your myopia is between –3 and –20 dioptres, or hyperopia up to +10 D, with or without astigmatism up to 6 D (Toric EVO ICL).
- Your anterior chamber depth is ≥2.8 mm and endothelial cell count is ≥2,200 cells/mm².
- Your cornea is too thin for LASIK, or you have moderate-to-severe dry eye that excludes flap-based refractive surgery.
- You want a reversible refractive option in case your visual needs change later (e.g. early cataract or presbyopia in your 50s).
A different pathway may be safer if
- Anterior chamber depth below 2.8 mm — risk of crowding and endothelial cell loss.
- Endothelial cell count below 2,200 cells/mm² — long-term lens tolerance compromised.
- Active iritis, uveitis or any uncontrolled intraocular inflammation.
- Cataract above an early stage — Smart Lens / cataract surgery is the more durable option.
- Narrow-angle glaucoma or untreated angle anatomy — risk of post-op intraocular pressure rise.
- Pregnancy or breastfeeding — ICL surgery is postponed.
Disclaimer. Information on this page is consistent with American Academy of Ophthalmology (AAO) Refractive Surgery Preferred Practice Pattern, American Society of Cataract & Refractive Surgery (ASCRS) consensus, FDA EVO ICL approval (March 2022, STAAR Surgical), and long-term FDA post-market safety data. It is educational and not a clinical recommendation. The only reliable way to know whether EVO ICL is the right option for you is a surgeon-reviewed evaluation based on biometry, anterior segment OCT, endothelial cell count and pupil dynamics — which is why our consultation is free of charge and free of obligation.
Realistic outcomes — the risks that actually matter
Every refractive procedure has measurable risks. We list them here in the same plain language our surgical team uses in your consultation:
Endothelial cell loss
Long-term studies (Alfonso et al. 2019; STAAR FDA post-market) show approximately 6 to 8 percent cell loss at 5 years — well within the acceptable safety threshold for the corneal endothelium. We monitor cell count at year 1 and annually thereafter.
Intraocular pressure rise
EVO ICL's CentraFLOW port largely eliminates the older Visian iridotomy requirement. Transient IOP spikes in the first 24 hours are uncommon (<3%) and resolve with topical medication. Long-term glaucoma risk is rare with proper anatomy screening.
Cataract development
Approximately 1–2% lifetime risk of anterior subcapsular cataract — typically late-onset (>10 years). The advantage of ICL is reversibility: if cataract develops, the ICL is removed and replaced with a Smart Lens / IOL in a single staged procedure.
Lens repositioning or exchange
Around 1% of patients require ICL repositioning or size exchange within the first year, typically because the initial sizing was at the borderline. Eyeglow includes one repositioning procedure within 12 months at no extra surgical fee.