Corneal Transplant & Keratoplasty in Turkey — DALK, PK and DMEK at Eyeglow Istanbul
Cornea-specialist-led transplant surgery using EBAA-graded donor tissue — Deep Anterior Lamellar Keratoplasty (DALK), Penetrating Keratoplasty (PK), and Descemet Membrane Endothelial Keratoplasty (DMEK). Every case reviewed by our cornea specialist team, with complication insurance, structured 12-month follow-up and a single named coordinator throughout.
Verified and listed across leading directories and authorities
What is corneal transplant surgery?
Corneal transplantation — keratoplasty — replaces damaged corneal tissue with EBAA-graded donor tissue to restore corneal clarity and visual function. Three techniques are used at Eyeglow Health: DALK (anterior stroma only, endothelium preserved), Penetrating Keratoplasty (full-thickness replacement), and DMEK (posterior Descemet layer and endothelium only) — matched to each patient's corneal pathology.
Corneal transplantation is indicated when disease, scarring or endothelial failure has reduced the cornea's optical clarity or structural integrity beyond what contact lenses, cross-linking, or ring segments can manage. At Eyeglow Health in Istanbul, every keratoplasty case is planned by our cornea specialist team using Pentacam Scheimpflug topography, anterior-segment OCT and specular endothelial cell count — consistent with American Academy of Ophthalmology (AAO) Preferred Practice Pattern on Corneal Edema and Opacification (2018), the Cornea Society Preferred Practice Patterns, NICE IPG585 (DMEK, 2017) and Eye Bank Association of America (EBAA) tissue standards.
Corneal transplant is a major intraocular surgical procedure with a defined recovery period (3 to 18 months depending on technique) and a lifelong steroid maintenance requirement. It is not appropriate for every patient with reduced corneal clarity. Active infection, uncontrolled glaucoma, severe posterior segment disease or poor ocular surface health must be addressed before transplant — and realistic visual prognosis is discussed frankly with every patient before the donor tissue request is filed.
From first consultation to graft maturation
- 01
Online cornea review and donor request
You share topography (Pentacam preferred), pachymetry maps, refraction history, slit-lamp photos or video, and the diagnosis confirmed by your local ophthalmologist. Our cornea specialist team reviews your case to confirm the diagnosis, whether the fellow eye is at risk, and which keratoplasty technique matches your corneal pathology — before a donor tissue request is filed with our partner eye bank.
- 02
Donor tissue and EBAA-grading confirmation
Donor corneas procured for our procedures are graded to Eye Bank Association of America (EBAA) criteria — specular endothelial cell count ≥2,000 cells/mm², age-appropriate tissue, no active infection and full donor serology. For DMEK, the Descemet membrane is pre-stripped by the eye bank to confirm peel integrity before the tissue is dispatched. Tissue availability typically requires 1 to 2 weeks notice; urgent clinical cases are prioritised.
- 03
Pre-operative imaging in Istanbul
Day 1 in Istanbul: Pentacam Scheimpflug topography, anterior-segment OCT (AS-OCT), specular endothelial cell count, slit-lamp biomicroscopy and biometry if IOL power calculation is needed (combined triple procedure). These confirm the correct technique, K readings, anterior chamber depth and the status of the fellow eye.
- 04
The procedure (about 1 hour)
DALK: the anterior 95% of the corneal stroma is removed using pneumatic deep dissection (big-bubble technique) or manual lamellar dissection, preserving the patient's Descemet membrane and endothelium. The donor stroma is sutured into place. DMEK: a thin scroll of donor Descemet membrane and endothelium only is injected into the anterior chamber through a small incision and unfolded with an air bubble — no sutures required in the cornea itself. PK: full-thickness donor button sutured with 16 or combined sutures; used when both stroma and endothelium are diseased or scarred to the visual axis.
- 05
Post-operative reviews and steroid management
DMEK patients return on day 1 for air-bubble position check; a second small air injection is available in clinic if needed. DALK and PK patients are reviewed on day 1 and day 5. Topical steroid drops (prednisolone acetate 1%) are prescribed long-term — typically one year or lifelong — to reduce rejection risk. A structured tapering protocol is provided in writing with your discharge summary.
- 06
One-year structured aftercare
Scheduled video reviews at one, three, six and twelve months. Slit-lamp photos, endothelial cell counts and Pentacam scans are repeated at each milestone to document graft clarity, cell density and rejection-free status. Suture removal timing (PK/DALK) is guided by topographic astigmatism, not fixed schedule. Your named coordinator manages the entire pathway.
DALK vs Penetrating Keratoplasty vs DMEK — which keratoplasty is right for you?
The keratoplasty technique is determined by which corneal layer is diseased. Here is how the three approaches differ in practice:
| Aspect | DALK | Penetrating Keratoplasty (PK) | DMEK |
|---|---|---|---|
| What is replaced | Anterior stroma only — Descemet + endothelium preserved | Full-thickness cornea — all layers | Descemet membrane + endothelium only |
| Ideal patient | Advanced keratoconus, stromal scarring, anterior dystrophies with healthy endothelium | Full-thickness stromal scarring, severe infections reaching endothelium, previously failed DALK | Fuchs endothelial dystrophy, bullous keratopathy, posterior corneal failure with clear stroma |
| Rejection rate | Endothelial rejection near zero (own endothelium retained); stromal rejection <5% | Endothelial rejection 10–20% at 5 years; immunosuppressive drops required lifelong | Rejection 1–4% at 5 years — substantially lower than PK; DMEK is the endothelial standard of care |
| Visual recovery | Best corrected vision returns at 6–12 months as astigmatism settles; spectacle correction still common | Best corrected vision at 12–18 months; irregular astigmatism requires rigid contact lens in many cases | Functional vision at 4–8 weeks; near-normal endothelial function within 3 months |
| Sutures | 16 interrupted or combined sutures — selective removal guided by topography | 16 interrupted or combined sutures — selective removal guided by topography | No corneal sutures — incision closed with 1–2 scleral sutures only |
| Donor tissue grading (EBAA) | Endothelial count ≥2,000 cells/mm² required; donor age and tissue thickness factor | Endothelial count ≥2,000 cells/mm²; whole-button prepared by eye bank | Endothelial count ≥2,500 cells/mm² preferred; Descemet pre-stripped and integrity confirmed before dispatch |
Corneal transplant pricing
All-inclusive Eyeglow package pricing. Your final, personalised quote is confirmed after imaging review — with no obligation.
| Procedure | Eyeglow price (all-inclusive) |
|---|---|
| Corneal Transplant (DALK / PK / DMEK) — per eye, donor tissue included, all-inclusive | €7,000 – €10,000 |
What's included in your corneal transplant package
Included in package
- Pre-op imaging (Pentacam topography, anterior OCT, specular endothelial count, slit-lamp, biometry)
- Cornea specialist team consultation + technique review
- Donor corneal tissue — EBAA-graded, full serological clearance
- DALK / PK / DMEK procedure including anaesthesia and theatre
- Day-case procedure — no overnight hospital stay
- 5-star hotel — 7 nights
- VIP airport transfers (return)
- Post-op drops kit (steroids, antibiotics, lubricants)
- Day-1, day-5, 1m, 3m, 6m, 12m review (slit-lamp + endothelial count + Pentacam)
- Multilingual cornea coordinator — 24/7
- Complication insurance policy (Türkiye Ministry of Health certified, covers surgical complications including infection, retreatment, and emergency intervention up to package value)
Paid separately
Items below are not part of the medical package — your coordinator helps arrange them at no markup.
- Flights to/from Istanbul
- Personal expenses
- Specialty rigid / scleral contact lens fitting after surgery (optional, quoted separately)
- Suture removal visits beyond the 12-month structured pathway (rare, case-by-case)
- Unrelated medical treatments
- Travel insurance (recommended — covers flight cancellation, baggage, non-surgical medical emergencies abroad; we coordinate referral if needed)
The surgeons who will care for you
Your procedure is carried out by our cornea specialist team at our partner accredited hospital in Istanbul. Their training and sub-specialty focus are shown below.
Medically reviewed by Assoc. Prof. Dr. Muhammet Derda Özer, FICO

Assoc. Prof. Dr. Muhammet Derda Özer, FICO
Operating Surgeon
Specialises in ocular oncology, vitreoretinal diseases, cataract, refractive, corneal transplantation, glaucoma and pediatric ophthalmic surgery — more than 30,000 ophthalmic operations across a 14-year clinical career.
View full profile
Op. Dr. Önder Aslan
Operating Surgeon
Board-certified ophthalmologist whose surgical practice spans anterior-segment procedures with oculoplastic and retinal sub-specialties — cataract, refractive, eyelid surgery and pediatric eye examinations including retinopathy of prematurity.
View full profile
Op. Dr. Muhammed Talha Sadık
Operating Surgeon
Board-certified ophthalmologist working across vitreoretinal disease, refractive, cataract and glaucoma surgery, with an active anterior- and posterior-segment surgical caseload.
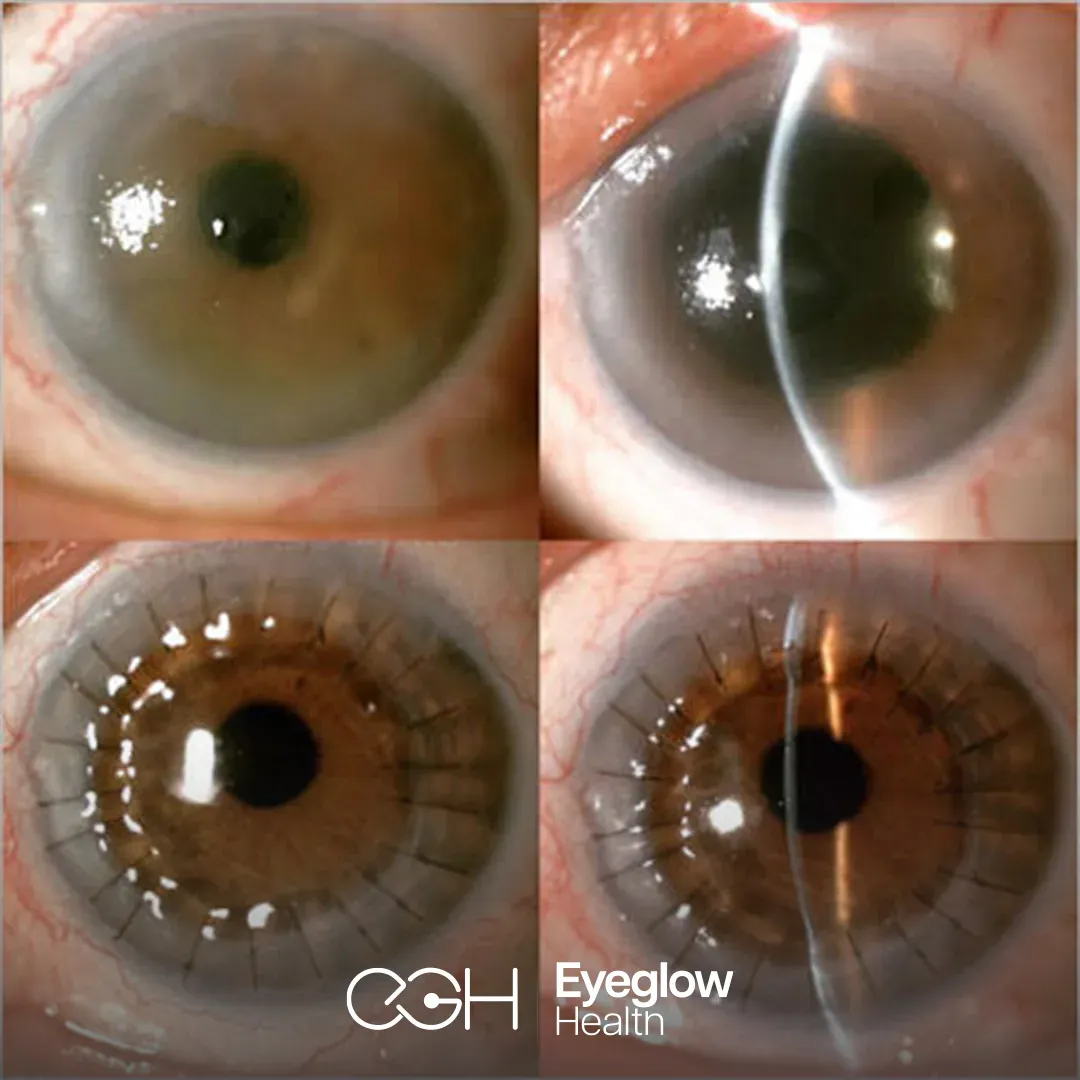
View full profileKeratoplasty outcomes from our own cases
The images below are from corneal transplant (keratoplasty) cases managed by our surgical team in Istanbul — documented before surgery and after graft healing. They are shared to illustrate the conditions our team treats, not as a guarantee of any individual outcome.
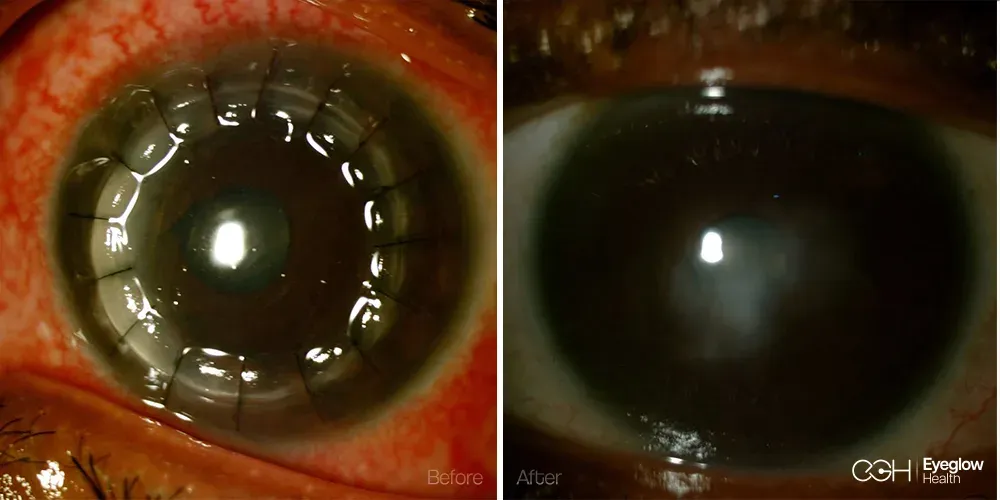
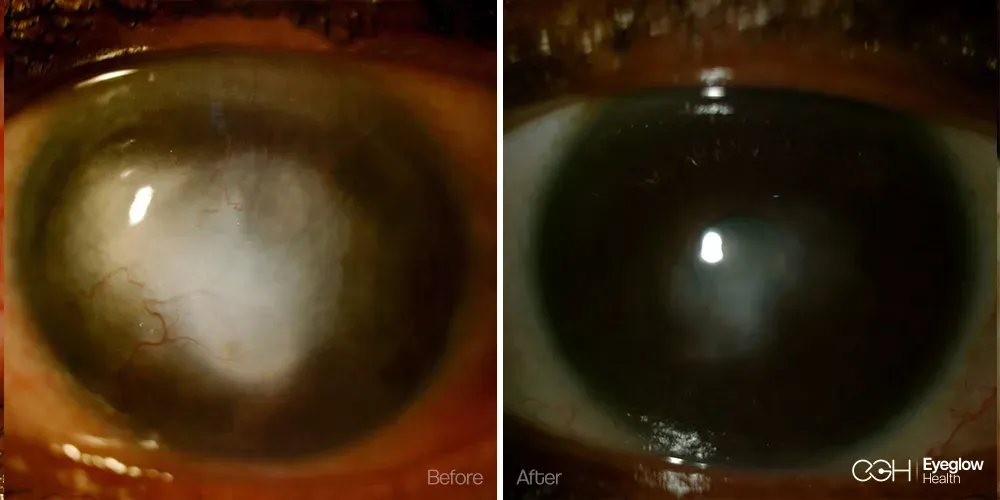
Clinical images are published with documented patient consent and are from procedures performed by our own surgical team. Individual results vary with corneal condition, graft type and healing; these images do not represent a promised result for any patient.
Are you a candidate for corneal transplant surgery?
You may be a good candidate if
- You have advanced keratoconus where cross-linking (CXL) has failed or is no longer suitable due to corneal thickness below 380 µm, or K-max has progressed to scarring despite prior treatment.
- You have Fuchs endothelial corneal dystrophy causing visual decline from endothelial cell failure and corneal oedema (bullous keratopathy).
- You have a corneal scar from prior infection (bacterial, fungal, herpetic) or injury that reaches the visual axis and reduces corrected vision below functional levels.
- You have corneal stromal oedema or decompensation following prior intraocular surgery (cataract, glaucoma shunts, vitreoretinal procedures).
- Your endothelial cell count is below 500 cells/mm² with progressive corneal thickening and recurrent episodes of painful bullous keratopathy.
- You have a congenital corneal opacity or anterior dystrophy with a healthy endothelium (DALK candidacy).
Surgery may need to be deferred or reconsidered if
- Active corneal infection (bacterial keratitis, fungal keratitis, acanthamoeba) — the infection must be fully resolved before transplant surgery is scheduled.
- Uncontrolled glaucoma with elevated intraocular pressure — IOP must be managed before transplant to protect the donor graft.
- Severe ocular surface disease (dry eye, lid malposition, cicatricial conjunctivitis) — surface health directly determines graft survival and must be optimised pre-operatively.
- Significant posterior segment disease (dense vitreous haemorrhage, proliferative retinopathy, severe macular disease) where corneal clarity alone will not restore meaningful vision — realistic visual prognosis must be established first.
- Patients with only one functioning eye require extended counselling and must weigh the risk of a period of reduced vision during recovery before agreeing to elective transplant.
Disclaimer. Information on this page is consistent with the American Academy of Ophthalmology (AAO) Preferred Practice Pattern on Corneal Edema and Opacification (2018), Cornea Society Preferred Practice Patterns, NICE Interventional Procedures Guidance IPG585 (DMEK, 2017), and Eye Bank Association of America (EBAA) tissue grading standards. It is educational and not a clinical recommendation. The only reliable way to determine whether DALK, PK or DMEK is appropriate for your corneal pathology is a specialist evaluation using Pentacam topography, AS-OCT, specular endothelial count and slit-lamp biomicroscopy — which is why our consultation is provided at no charge and without obligation.
Realistic outcomes — the risks that matter
Corneal transplant is a major surgical procedure. Our cornea specialist team explains these risks in full during the pre-operative consultation; they are listed here in the same plain terms:
Immunological rejection
Endothelial rejection occurs in 10 to 20 percent of PK cases at 5 years, under 4 percent with DMEK, and near zero for the endothelial layer with DALK. Rejection presents as pain, redness, photophobia and sudden vision blurring — it is a medical emergency. Early intensive topical steroid treatment reverses most rejection episodes when started within 24 hours of symptom onset. Patients receive a written rejection symptom card at discharge.
Primary graft failure
About 2 to 5 percent of donor grafts fail to function within the first week despite technically correct surgery — a consequence of donor tissue quality or undetected endothelial compromise. EBAA-graded tissue with pre-operative endothelial count reduces but does not eliminate this risk. Regrafting is the established management.
Graft infection
Post-keratoplasty infectious keratitis occurs in under 2 percent of cases. Risk is highest in the first month during epithelial healing. Prophylactic topical antibiotics are prescribed for the first month; any new pain, discharge or infiltrate is evaluated as urgent.
Elevated intraocular pressure
Post-keratoplasty steroid response (raised IOP from long-term steroid drops) occurs in 20 to 35 percent of patients. IOP is monitored at every follow-up visit; a topical IOP-lowering agent is added when pressure exceeds 21 mmHg. Steroid responders are identified early and managed to protect the optic nerve.
Irregular astigmatism (PK / DALK)
Full-thickness and lamellar transplants heal with variable corneal curvature — irregular astigmatism of 3 to 6 dioptres is common. Spectacles or rigid gas permeable contact lenses provide good correction in most cases; selective suture removal and corneal relaxing incisions are used when topography-guided adjustment is appropriate. Visual rehabilitation typically takes 12 to 18 months after PK.