Gastric Bypass in Turkey — Roux-en-Y and Mini Gastric Bypass at Eyeglow Istanbul
Laparoscopic Roux-en-Y or mini gastric bypass — small stomach pouch plus intestinal rerouting combines restriction and malabsorption. 70–80% excess weight loss at 5 years and 60–70% type 2 diabetes remission per IFSO global registry. Bypass is the preferred bariatric procedure for severe GERD, large hiatus hernia, and insulin-dependent or long-duration type 2 diabetes. Performed at our partner accredited hospital by a board-certified bariatric surgeon, with full pre-op workup, intra-op leak test, and 12-month structured nutritional follow-up.
Verified and listed across leading directories and authorities
What is gastric bypass surgery?
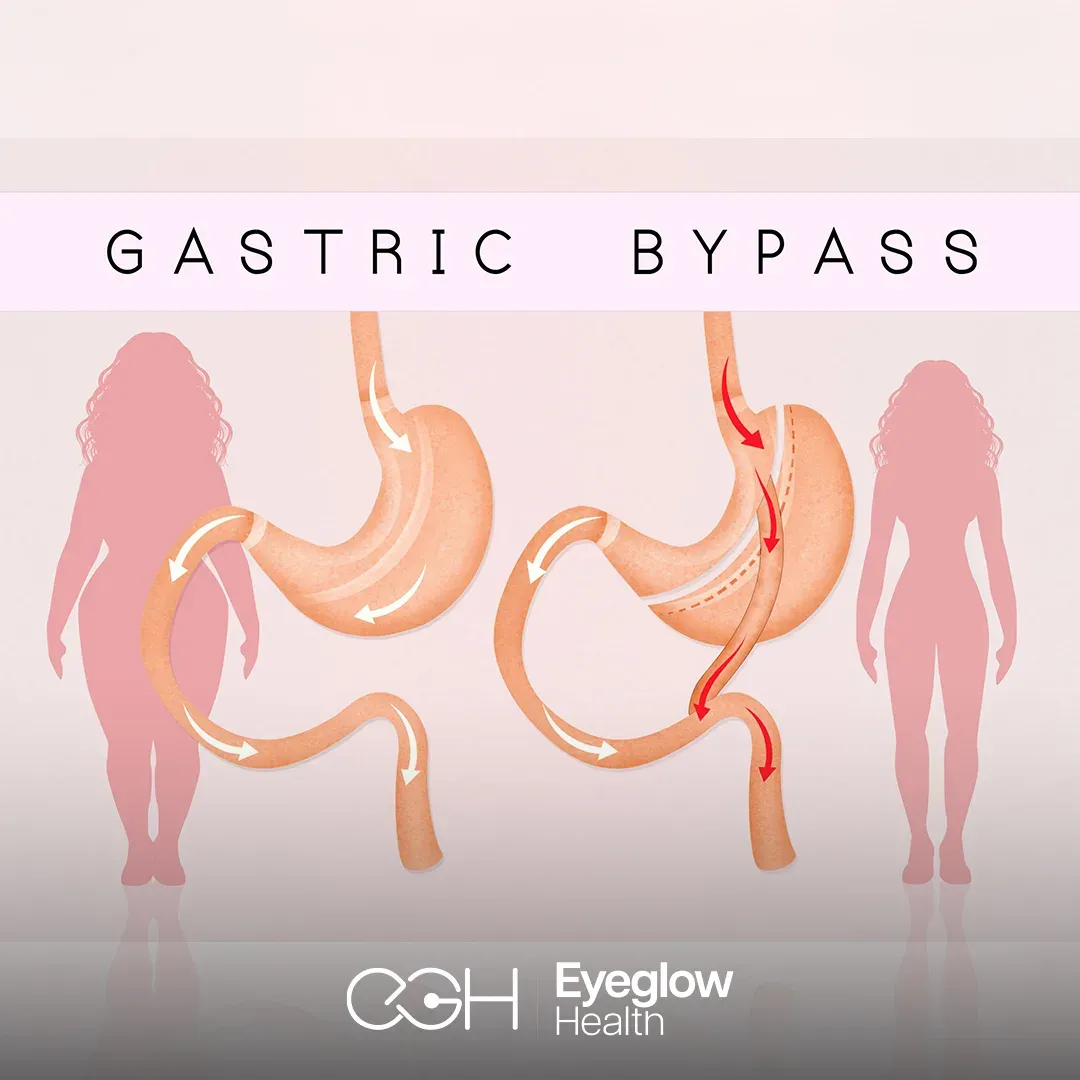
Gastric bypass — most commonly Roux-en-Y gastric bypass (RYGB) — is a bariatric procedure combining restriction and malabsorption. A small (~30 ml) proximal stomach pouch is created and connected via a Y-shaped intestinal reconstruction that bypasses the duodenum and proximal jejunum. Mini gastric bypass (MGB / OAGB) is a single-loop variant with similar outcomes. Per IFSO global registry: 70–80% excess weight loss at 5 years, 60–70% type 2 diabetes remission, and reflux improvement.
At Eyeglow Health in Istanbul, gastric bypass is performed at our partner accredited hospital by a board-certified bariatric surgeon holding IFSO-recognised credentials with documented bypass volume. The Turkish Ministry of Health International Health Tourism Authority Certificate is held by both Eyeglow and the partner hospital. We follow IFSO and ASMBS guidelines for candidate selection, pre-operative workup, intra-operative protocol (anastomotic leak testing, mesenteric defect closure) and structured follow-up.
Bypass is the right procedure for patients with severe pre-existing GERD or large hiatus hernia, insulin-dependent or long-duration type 2 diabetes, or BMI >50 where durable loss matters most. It is not the right choice for patients with prior extensive bowel surgery, Crohn\'s disease, or those unable to commit to lifelong nutritional supplementation. That decision belongs to a bariatric surgeon who has personally reviewed your full medical history — not to a marketing brochure.
From eligibility review to 12-month follow-up
- 01
Online eligibility review + BMI + comorbidity screen
You share your height, weight, BMI, medical history (type 2 diabetes, hypertension, sleep apnoea, GERD, joint disease), reflux symptoms and medication list. The bariatric surgeon checks IFSO/ASMBS criteria — BMI ≥40, or BMI ≥35 with at least one comorbidity, with bypass often preferred over sleeve when severe GERD, hiatus hernia, BMI >50 or insulin-dependent type 2 diabetes is present. If you do not meet criteria we tell you honestly before any package is quoted.
- 02
Pre-operative tests in Istanbul (day 1)
Full blood panel (CBC, INR, HbA1c, lipid profile, liver and kidney function, thyroid, vitamin D, B12, ferritin, iPTH), upper-GI endoscopy (to assess hiatus hernia, GERD severity, exclude Helicobacter pylori, ulcer or undiagnosed pathology), abdominal ultrasound (gallbladder evaluation — rapid weight loss increases gallstone risk), ECG, chest X-ray, anaesthesia review and pulmonary clearance. Pre-op liver-shrinking diet of 10–14 days is started before you fly.
- 03
Surgeon consultation + procedure selection (RYGB vs MGB)
The bariatric surgeon walks you through Roux-en-Y vs mini gastric bypass selection — RYGB is the gold-standard 60-year-tested technique with Y-shaped intestinal reconstruction; MGB (one-anastomosis) is faster, technically simpler, with one anastomosis instead of two, and similar weight-loss outcomes but slightly higher bile reflux risk. The surgeon discusses expected weight-loss curve (70–80% excess weight loss at 5 years per IFSO registry), diabetes remission (~60–70%), lifelong nutritional supplementation, the irreversible nature in practice, and realistic risks.
- 04
Laparoscopic gastric bypass (90–150 minutes)
Under general anaesthesia, 4–6 small abdominal incisions are used for laparoscopic access. RYGB: a small (~30 ml) proximal stomach pouch is created and separated from the remainder of the stomach. The jejunum is divided ~50 cm distal to the duodenojejunal junction; the distal limb (alimentary limb, ~75–150 cm) is anastomosed to the pouch (gastrojejunostomy); the proximal limb (biliopancreatic limb, carrying bile and pancreatic juice) is reconnected further down (jejunojejunostomy), creating a Y-shape. MGB uses a longer gastric pouch with a single loop gastrojejunostomy. Anastomoses are tested intra-operatively.
- 05
Hospital recovery + contrast study + discharge (3–5 nights)
Day 1 post-op: clear liquid intake under nursing supervision, early mobilisation to reduce DVT risk, IV proton-pump inhibitor and analgesia. Day 2: upper-GI contrast study confirms no anastomotic leak; clear liquid diet continues. Days 3–5: progressive diet, drain removal if used, dumping-syndrome counselling, discharge planning to your 5-star hotel on a purée diet protocol with detailed daily volume guidance.
- 06
12-month structured nutritional follow-up
Diet stages: clear liquids (week 1) → full liquids (week 2) → purée (weeks 3–4) → soft food (weeks 5–6) → solid food from week 7. Scheduled video reviews at 1, 3, 6 and 12 months covering weight-loss curve, nutritional bloods (B12, iron, folate, calcium, vitamin D, iPTH, zinc), supplement compliance, comorbidity improvement (HbA1c, blood pressure, GERD resolution), dumping-syndrome management and psychological adjustment. Lifelong nutritional supplementation is essential and we explain why honestly.
Gastric bypass vs sleeve vs balloon vs lifestyle
Bariatric surgery is not the right answer for every patient with obesity. Here is how the four main pathways compare:
| Aspect | Gastric bypass | Gastric sleeve | Gastric balloon | Lifestyle + medication |
|---|---|---|---|---|
| Mechanism | Restriction + malabsorption (intestinal rerouting) | Restriction + ghrelin reduction | Restriction (temporary, 6–12 months) | Behavioural — diet + exercise + medication |
| Reversibility | Reversible in principle; rarely reversed in practice | Irreversible (stomach removed) | Removed at 6–12 months | Fully reversible |
| Excess weight loss (5y) | 70–80% | 60–70% | 15–25% (during balloon period) | 5–10% (most patients regain) |
| Diabetes T2 remission | 60–70% | 50–60% | Limited | <10% |
| GERD outcome | Improves reflux (preferred for severe GERD) | Often worsens reflux | May worsen reflux | Depends on weight loss |
| Hospital stay | 3–5 nights | 3 nights | 0–1 night | None |
| Nutritional risk | High (malabsorption — lifelong supplements + annual bloods mandatory) | Moderate (B12, iron, calcium) | Low | None |
Personalised pricing
Every treatment plan is priced individually after your consultation. Request a written, all-inclusive quote — clear, itemised, and with no obligation.
Request a written quoteWhat's included in your gastric bypass package
Included in package
- Pre-op bariatric surgeon consultation + IFSO/ASMBS eligibility review
- Full blood panel + upper-GI endoscopy + abdominal ultrasound + gallbladder assessment + ECG + chest X-ray
- Anaesthesia review + pulmonary clearance
- Laparoscopic gastric bypass (RYGB or MGB) at partner accredited hospital
- General anaesthesia + intra-op anastomotic leak test
- Hospital stay — 3 to 5 nights private room
- 5-star hotel — 2 to 3 nights post-discharge
- VIP airport transfers + hospital-hotel transfers
- Post-op contrast study (upper-GI X-ray) before discharge
- All post-op medications + proton-pump inhibitor + DVT prophylaxis + dietitian-led nutritional kit + dumping-syndrome guidance
- 1, 3, 6 and 12-month video nutritional follow-up + bloods interpretation
- Multilingual bariatric coordinator — 24/7 throughout your stay
- Complication insurance — covers eligible post-operative medical complications during the recovery period at our partner accredited clinic (issued in line with the Turkish Ministry of Health International Health Tourism Authority Certificate)
Paid separately
Items below are not part of the medical package — your coordinator helps you arrange them at no markup.
- Flights to/from Istanbul
- Personal expenses + food after discharge
- Lifelong nutritional supplements (bariatric multivitamin, B12 sublingual or injection, calcium citrate + vitamin D, iron, folate — prescribed at discharge)
- Local-country dietitian follow-up after the 12-month package ends
- Plastic surgery for post-weight-loss skin laxity (abdominoplasty, brachioplasty, mastopexy — quoted separately)
- Cholecystectomy if gallstones develop during rapid weight loss (typically months 3–12)
- Travel insurance (flight cancellation, baggage, general trip cover) — separate from the medical complication policy above; your coordinator can recommend a provider at no markup
Are you a candidate for gastric bypass?
You may be a good candidate if
- Your BMI is 40 or above, or 35 or above with an obesity-related comorbidity (type 2 diabetes, hypertension, obstructive sleep apnoea, severe joint disease, NAFLD) per IFSO/ASMBS guidelines.
- You have severe GERD (reflux), large hiatus hernia, or Barrett's oesophagus — bypass improves reflux while sleeve typically worsens it.
- You have insulin-dependent or long-duration type 2 diabetes — bypass has the highest diabetes remission rate of any bariatric procedure (60–70% at 5 years per IFSO data).
- You understand the procedure carries permanent malabsorption and accept lifelong nutritional supplementation with annual blood monitoring.
- You are willing to commit to staged diet progression, 12-month structured follow-up, and dumping-syndrome dietary discipline (no high-sugar or high-fat meals).
Bypass is not the right choice if
- Your BMI is below 35 without an obesity-related comorbidity — bypass is not indicated; consider medical management (GLP-1 RA, behavioural therapy) or a less invasive procedure.
- You have Crohn's disease, prior extensive small bowel resection, or known short-bowel risk — malabsorption procedure is contraindicated.
- You are unwilling or unable to commit to lifelong vitamin/mineral supplementation, sublingual or injected B12, and annual nutritional bloods.
- You have an active untreated eating disorder or substance use disorder — psychiatric stabilisation required first.
- You are pregnant, breastfeeding, or planning pregnancy within 18 months — defer surgery until pregnancy plans are completed (post-bypass pregnancy carries higher nutritional risk).
Disclaimer. Information on this page is consistent with IFSO (International Federation for the Surgery of Obesity), ASMBS (American Society for Metabolic and Bariatric Surgery) and NICE bariatric guidelines, and Turkish Ministry of Health International Health Tourism Authority Certificate requirements. The choice between bypass, sleeve, balloon and medical management is a case-by-case clinical decision based on BMI, comorbidities, reflux history and surgeon assessment — not a marketing-driven default.
Realistic outcomes — the risks that actually matter
Every bariatric procedure has measurable risks. We list them here in the same plain language our bariatric surgeon uses in your consultation:
Anastomotic leak (~1–2%)
A leak from the gastrojejunal or jejunojejunal anastomosis is the most serious bypass-specific early complication, occurring in approximately 1–2% of cases per IFSO global registry. Most leaks are detected by intra-op test or post-op contrast study before discharge. Late leaks (days 5–14) may present with fever, tachycardia, abdominal pain or shoulder-tip pain — patients are briefed to recognise these signs and contact the coordinator immediately. Management ranges from percutaneous drainage and endoscopic stenting to re-operation. Our partner hospital uses intra-operative leak testing and post-op contrast studies as standard.
Dumping syndrome (10–50% of bypass patients)
Dumping syndrome is the rapid emptying of unprocessed food from the small gastric pouch into the small intestine, triggered by high-sugar or high-fat meals. Early dumping (within 30 minutes): nausea, sweating, palpitations, abdominal cramps, diarrhoea — caused by osmotic fluid shift. Late dumping (1–3 hours): reactive hypoglycaemia, weakness, sweating — caused by insulin overshoot. Most patients learn to avoid trigger foods within months. Dumping is unique to bypass (not sleeve) and is sometimes considered a useful "behavioural enforcer" against sugar — but it can be distressing and we discuss it explicitly in consultation.
Internal hernia (~3% lifetime risk)
Bypass creates new spaces between intestinal mesenteries (Petersen's defect, mesenteric defect) where bowel can herniate later — typically months to years after surgery, often after significant weight loss creates more abdominal space. Symptoms: severe abdominal pain, vomiting, bowel obstruction. This is a surgical emergency requiring prompt diagnosis (CT scan) and laparoscopic repair. Modern technique closes mesenteric defects intra-operatively, reducing but not eliminating the risk. Lifelong awareness is required and patients are briefed to seek emergency care for severe persistent abdominal pain at any time after bypass.
Nutritional deficiency (high lifelong risk)
Bypass causes permanent malabsorption — particularly of iron, vitamin B12, calcium, vitamin D, folate and fat-soluble vitamins. Without rigorous lifelong supplementation, patients develop anaemia, osteoporosis, peripheral neuropathy, hair loss and protein malnutrition. Mandatory: bariatric-formulated multivitamin daily, sublingual or injected vitamin B12 (terminal ileum absorption pathway is bypassed), calcium citrate with vitamin D, iron if menstruating or anaemic, annual nutritional bloods for life. Bypass is not a procedure for patients who will skip supplements — the malabsorption is permanent and irreversible.